
Introduction
HP is the art of how the world affects your work, and how your work affects the world.
"People ignore design that ignores people" - Frank Chimero.
We are iGEM-ZJU winter project group 2 and we try our best to do the human practice part as well as we can in a month's time , showing the potential of our group. Despite the short time we had, we worked hard on many tasks that helped us to refine our project design and created opportunities for our project to have an impact on the world.
At the beginning of the project, we conducted a Stakeholder map brainstorm and a mendelow matrix value analysis to open up ideas for the human practice. When selecting topics and wavering over the direction of innovation, we honestly consulted several professors from Zhejiang University who encouraged our ideas and affirmed our creativity. The professors were delighted to receive our letter and offered suggestions. The advice was concise, and it was of great benefit to us.
The positive impact of Human practice on the project is undeniable and we plan to talk and communicate with more Stakeholders, which can be seen in our future plan.
We have tried to optimize and improve our project in a month and look forward to making an impact on the world through our work. We designed a questionnaire fitting the theme of the project and distributed it to the public. We were surprised to receive 178 answers to the questionnaire, which reflected the interest in the theme of our project. After realizing the lack of public knowledge in the field of diabetic foot, we created and wrote targeted educational tweets. The tweets included information on the prevention of diabetic foot, an introduction to iGEM and synthetic biology, and an introduction to GluLeaves , which received a high number of views. And we are very pleased about it. We look forward to doing more work that will benefit the world in the future.
We saw the possible business value of our project and designed a business plan for it, which is reflected in our Entrepreneurship part. In order to make a better mature plan for our startup, we would like to interact with other companies incubated on the Zhejiang University Entrepreneurship Platform and learn from experienced entrepreneurs and investors.
Detailed
Overview
Timeline
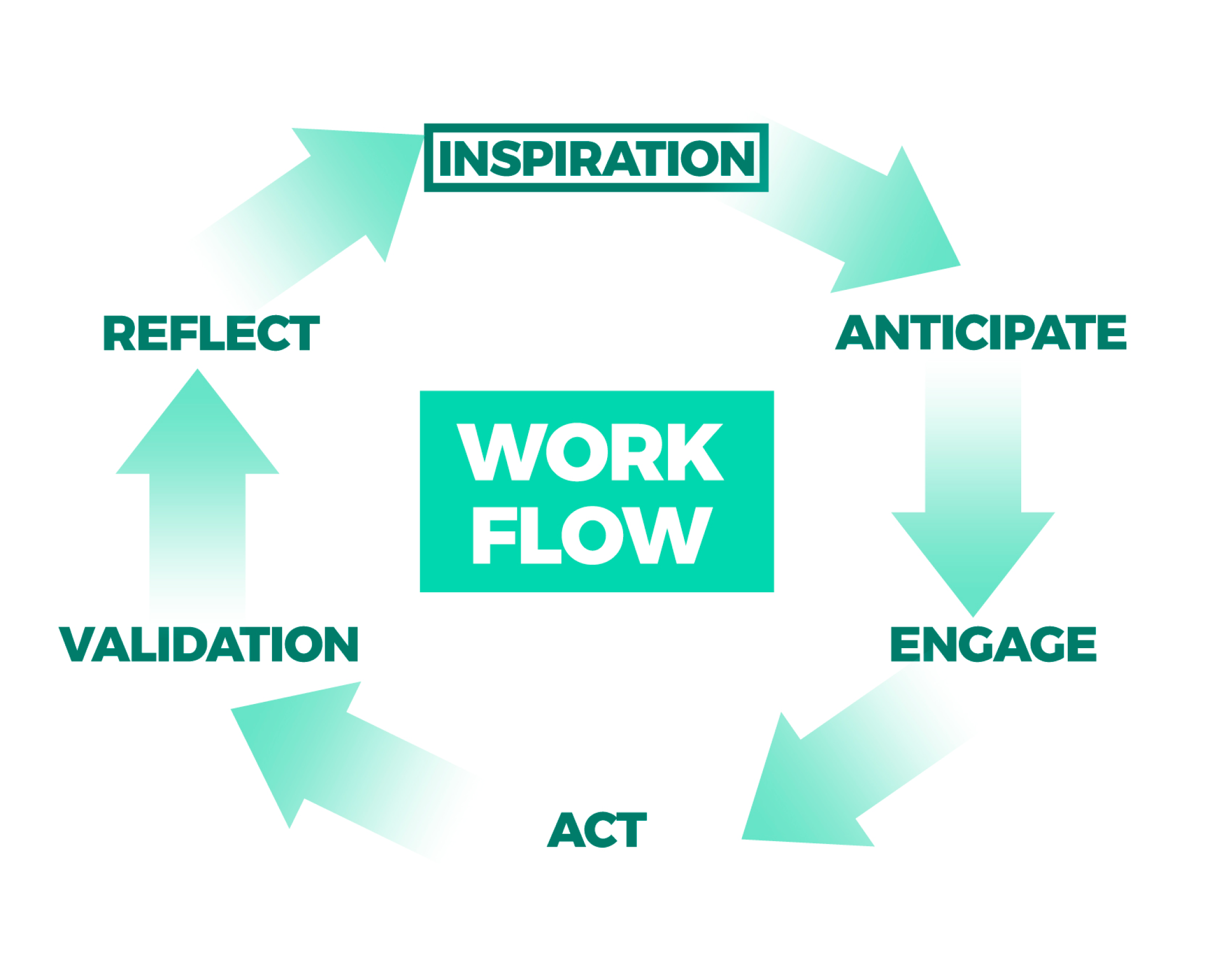
In order to make our human practice more efficient and Standardized, we have designed a project-specific workflow framework to support our project design and human practice. This workflow framework supports us in the design of our projects and the development of our human practice, which can be found in the Idealting section.
Understanding
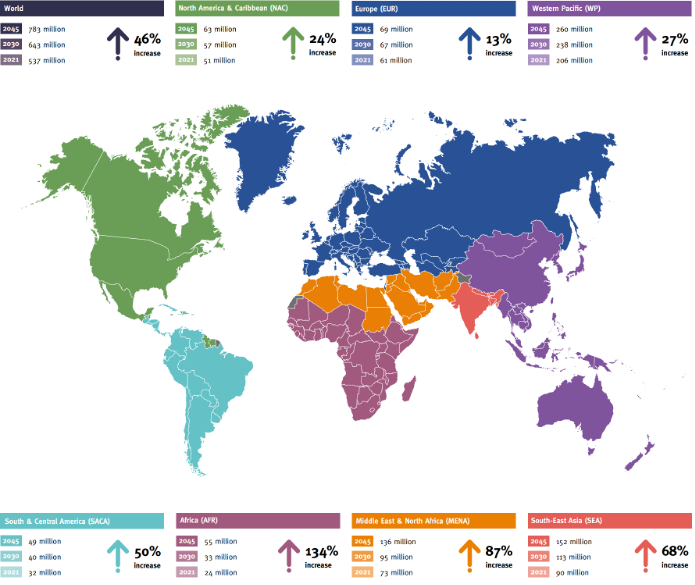
Diabetes is a major cause of lower limb amputation. Prevalence has been rising more rapidly in low- and middle-income countries than in high-income countries. The IDF Global Diabetes Map (10th Edition) states that diabetes is the fastest growing global health emergency of the 21st century. The data shows that the number of adults with diabetes reaches 537 million (10.5%) globally in 2021, with around one in ten adults affected. This is an increase of 74 million people, or 16%, compared to 2019, highlighting the alarming increase in the global prevalence of diabetes. The IDF speculates that this number will reach 783 million by 2045, a 46% increase that is more than double the estimated population growth (20%) over the same period, with the proportion of adults with the disease potentially reaching one in eight. Direct medical expenditure due to diabetes is already approaching US$1 trillion. In summary, current data suggest that the prevalence of diabetes remains on the rise globally and is increasing significantly, and that the health burden of diabetes remains a major challenge for individuals, families and societies.
At the NCRC-IM Forum on 15 January 2022, experts provided an analysis of the diabetic foot. With the gradual increase in the prevalence of diabetes in China, the prevalence of one of its most serious complications, the diabetic foot, is also increasing year by year. Among diabetic patients over 50 years old in China, the 1-year new incidence rate of diabetic foot is 8.1%, the 1-year mortality rate is 14.4% and the overall amputation rate is 19.3%. Ge Junbo, academician of the Chinese Academy of Sciences, director of the Department of Cardiology at Zhongshan Hospital of Fudan University and director of the National Clinical Medical Research Centre for Radiology and Therapeutics, pointed out that the treatment of diabetic foot is not simply about treating the foot, but also about managing the patient as a whole for the disease and focusing on the treatment of systemic diseases. In recent years, significant progress has been made in the interventional treatment of diabetic foot, but there are still many bottlenecks, and it is for this reason that it is worthwhile to keep exploring. We hope that in the future, we will form a closed-loop management from upstream prevention, treatment to post-operative rehabilitation, truly improving the quality of life of patients and allowing them to live with more dignity, which is the ultimate pursuit of medicine.
It is estimated that 1 diabetic amputation occurs every 20 seconds worldwide. People with diabetes are 10 to 20 times more likely to have their limbs amputated compared to normal people. One in seven diabetic patients has a foot ulcer.
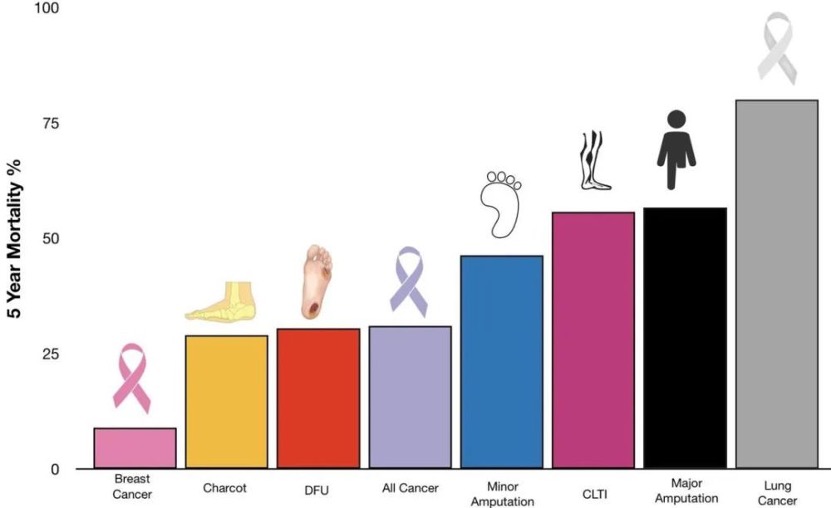
A 2013 study by Fortington [1] found that the life expectancy of patients after lower limb amputation was significantly shorter, with nearly one quarter dying within 30 days of amputation, nearly half dying within 1 year of amputation and up to 80% dying within 5 years of amputation; the 5-year survival rate for patients after lower limb amputation was lower than that of patients with general cancer. a 2020 study[2] showed that the 5-year mortality rate (attached) and direct care costs for patients with diabetic foot complications were comparable to those of cancer. Data from a European multicentre study[3] estimated the annual cost of treating diabetic foot ulcers to be as high as US$13,561 per capita, with the per capita cost of amputation in developed countries ranging from US$35,000 to US$45,000. A survey in China showed that the average per capita hospital cost for diabetic foot patients was approximately $15,000 in 2004, increasing to approximately $17,000 in 2012, and the median per capita hospital cost for amputation was $26,000. These results show that diabetic foot places a heavy medical and financial burden on diabetic patients, their families and society. Behind every case of diabetic foot disease is a family and a small community.
At the EASD Annual Meeting 2021, Professor Kristien Van Acker from Belgium presented on the epidemiology of the diabetic foot and future perspectives. She quoted Dr Connor's comment that "despite the recognition of the epidemiology of the diabetic foot and its relationship to diabetes in the 19th century, little progress was made in the treatment of diabetic foot ulcers in the first half of the 20th century".
Seeing the tremendous pressure that the diabetic foot places on patients and society, we decided to contribute to the treatment options for the diabetic foot .
Stakeholder Analysis
Stakeholders' critical perspectives on our ideas and feedback have helped us to optimise our project plans and solution designs to be effective, feasible. For an innovation project, it is important to connect with enough stakeholders and get their suggestions and feedback to reconsider and make improvements in the project. Only then is it possible to produce a human-centred design.
Therefore, we did a stakeholder brainstorm after we had decided on a topic. On the evening of Jan.31st we had this discussion online in 20 minutes. Before the brainstorming session, we prepared a document to introduce the concept of stakeholders, the concept and rules of the brainstorming session and the intended objectives of the brainstorming session to the team. The thorough preparation ensured that our three activities ran smoothly and successfully.
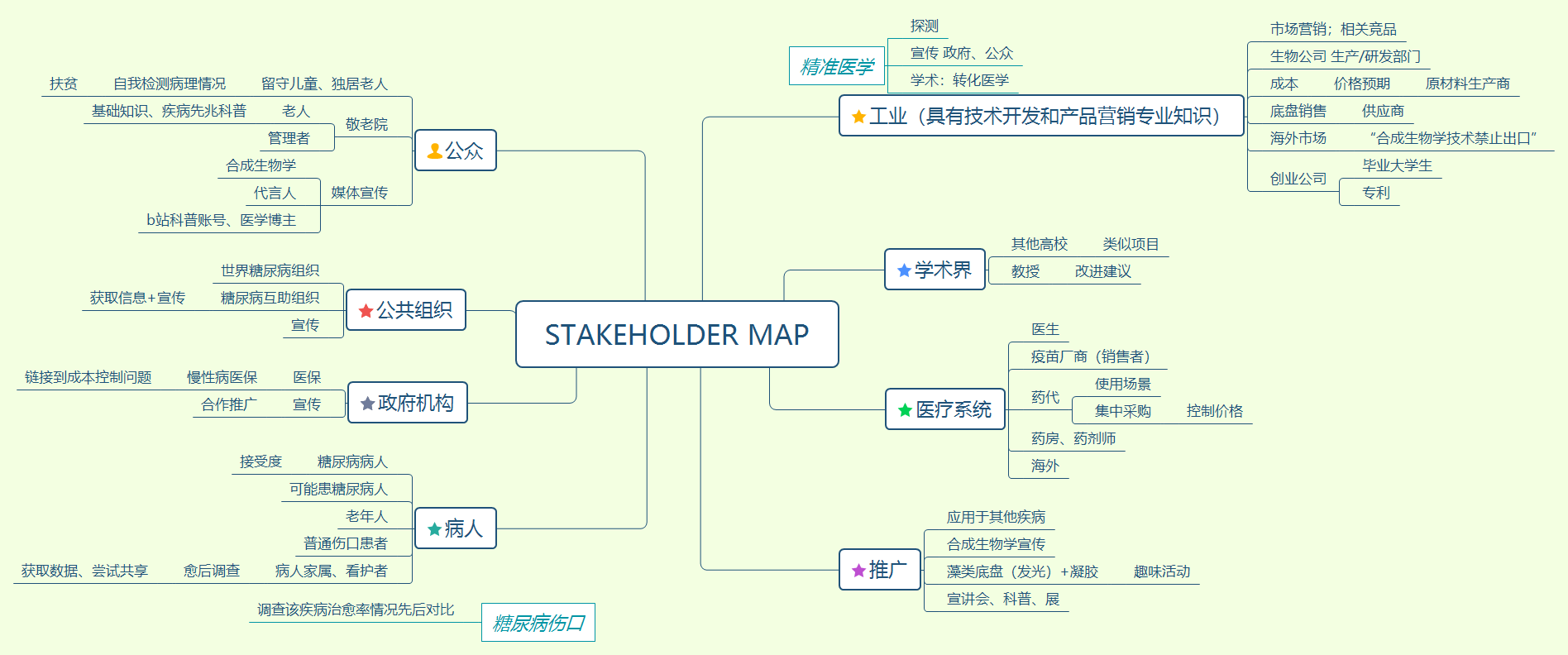
We have compiled and visualised the final results of the Stakeholder Map and Mendelow matrix value analysis.
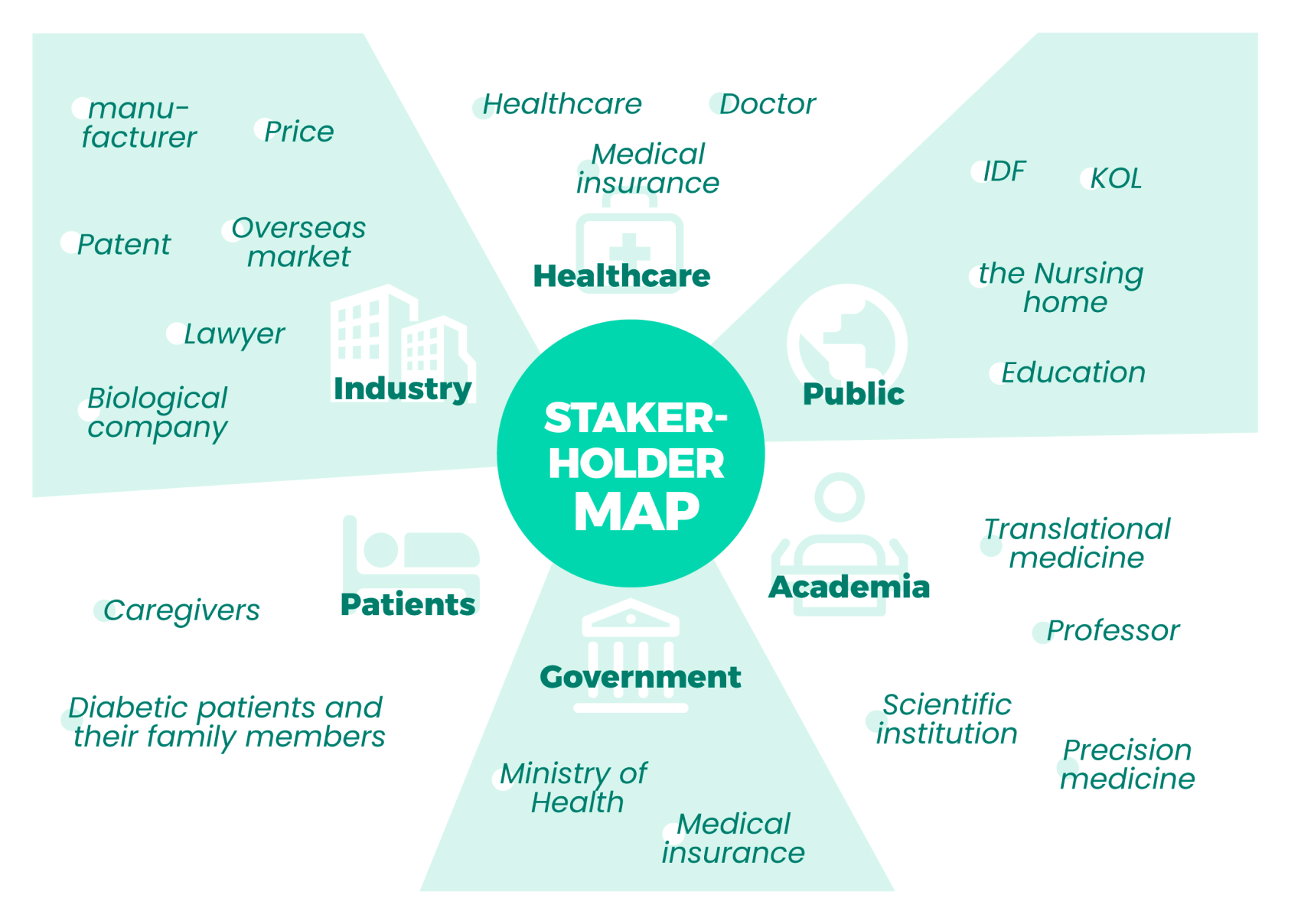
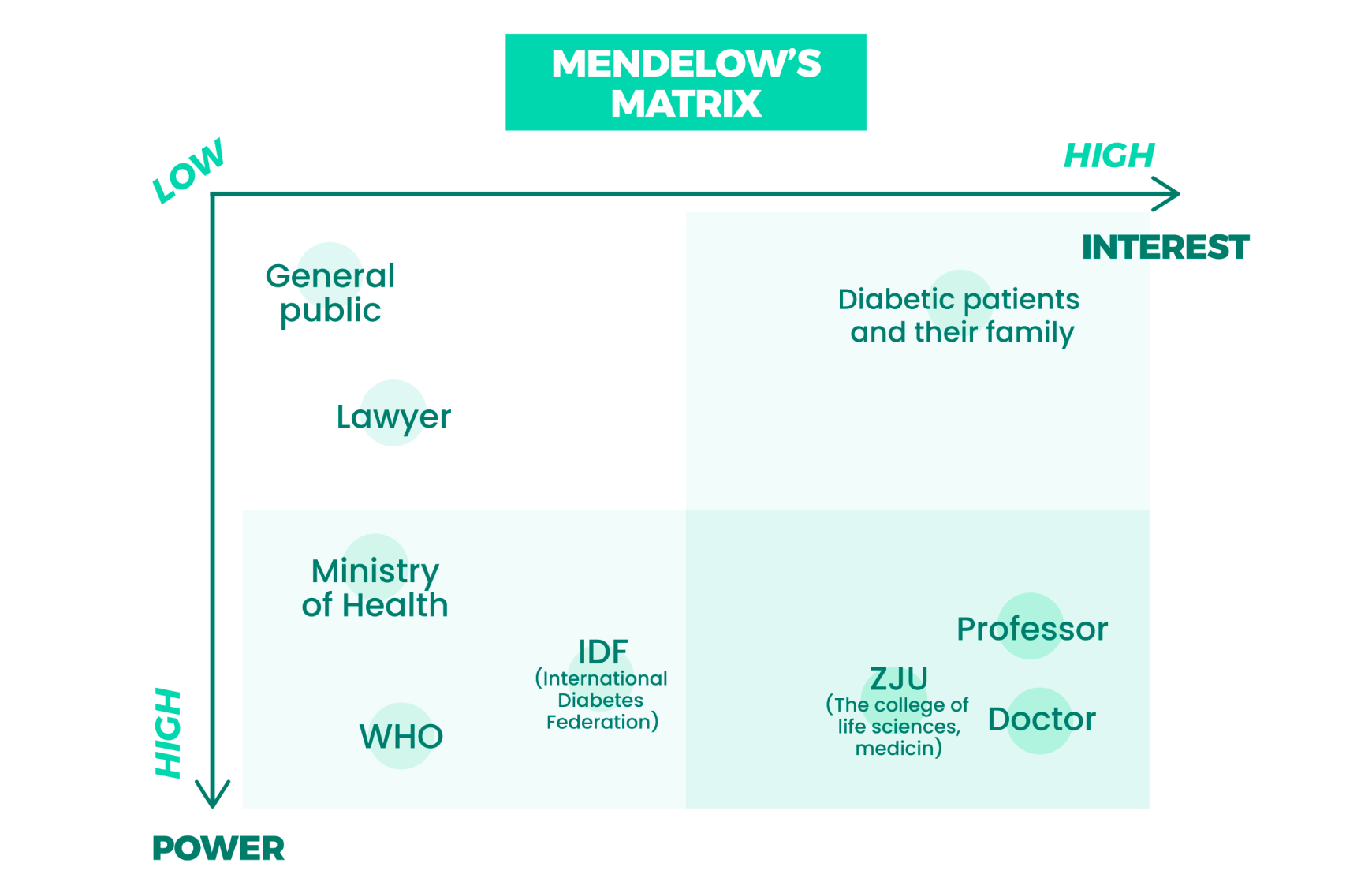
We have decided to focus on contacting High-Interest&Power stakeholders. At the same time, we will decide how often, for what purpose and how we work with different stakeholders depending on where they are in the matrix.
Ideating
I. Project Selecting
At the beginning of the project selection phase, our idea was to design a type of bio-dressing product that would be more relevant to the general public to relieve the more common, "less serious but more torturous" chronic wounds such as mouth ulcers or dental injuries.
But as the discussion progressed, we noticed a wound type that is more pernicious and serious in treatment today - diabetic chronic wounds. The number of diabetic patients in China has reached more than 100 million, about 25% of which are affected by diabetic foot [4]. Diabetic foot (DFU) is a foot infection, ulcer, and deep tissue destruction in diabetic patients due to distal nerve abnormalities and varying degrees of vasculopathy in the lower extremities and is among the most common types of diabetic chronic wounds, which may need amputation in severe cases.
Treatment of diabetic chronic wounds at late stages of development is quite difficult, but surveys have shown that in more than two-thirds (84%) of non-traumatic lower limb amputations due to diabetic foot, patients develop ulcers upfront [5], which opens a window for early intervention. Therefore, the direction of our project focused on the treatment of early diabetic foot ulcers.
II. Background Investigation
As a result of our investigation, the reasons for the difficulty in diabetic wound healing include: a sugar-rich tissue environment provides a medium for bacterial proliferation, the chronic release of pro-inflammatory factors, ischemia and hypoxia in the wound due to peripheral vascular disease, and neuropathy leading to poor patient awareness of the extent of wound development. [6]
We hope to gain a clearer understanding of the hierarchical relationship between the various factors that contribute to non-healing diabetic wounds and provide patients with treatment options that address both the symptoms and the root cause. After our further investigation, we targeted the key class of molecules, AGEs, which have been shown to be associated with vascular/neuropathy, excessive inflammatory response, and lack of growth factors at the wound [7] [8], and reducing the effective concentration of AGEs at the wound can alleviate the vascular neuropathy [8]. We, therefore, hope to use AGEs inhibitors, growth factors and antimicrobial substances acting together to promote wound healing.
III. Main Module Design
Next, our exploration proceeded in parallel with the selection of chassis cells and effector molecules. For the chassis cells, we proposed the idea of stem cells combined with exosomes for drug delivery, but the idea was abandoned due to the difficulty of obtaining stem cells and the harsh preservation conditions, which posed a challenge to the mass production of our products. After that, Chlamydomonas reinhardtii came into our vision. The advantage of the algal chassis is autotrophy, which means we do not need to add nutrients to the dressing, making it less susceptible to bacterial attack; in addition, the oxygen produced by the photosynthesis of C.reinhardtii can alleviate wound hypoxia.
For effector molecules, it has been shown that soluble AGEs receptor (sAGER) expression in mice significantly reduces inflammation and vascular complications [9], and we decided to use sAGER as a blocker of AGEs-receptor binding. Since various types of growth factors play redundant roles in wound healing and inflammatory responses, we selected a representative one, hEGF. For antimicrobial substances, we choose AMP LL37 for its promising behavior in fighting bacterial infections.
We encapsulated the above components into a therapeutic module. We tried to construct a negative feedback release regulation mechanism, but the idea was abandoned because the pathway design for sensing the concentration of AGEs in the environment was too complex, and the constitutive promoter was used instead to control the expression of the three effector molecules.
IV. Reporting and Biosafety Design
After completing the design of the main module, we started to think about the functionality and biosafety of the final product and designed the reporting module and the biosafety module.
The idea of the reporting module was initially proposed because of the patient's unclear understanding of the disease process due to possible neuropathy. At first, we wanted to report to the patient on the treatment of the wound by detecting the concentration of inflammatory factors at the wound, but again due to the difficulty of implementing the pathway, we switched the idea to have the dressing report only two states: a signal when the dressing is working and another signal when the wound deteriorates due to severe bacterial infection. We linked the luciferase gene downstream of the promoter of the therapeutic module and designed a sensing system to detect the AHL signal of P. aeruginosa at the wound to achieve our goal.
However, the ensuing problem is that only a few cells in the lower layer of the dressing can contact the wound and the concentration of reporter molecules produced when an infection occurs is too low to be detected. Therefore, we designed a quorum sensing module, where just a few cells receiving AHL molecules will cause all cells to initiate reporting together, giving a strong danger indication to the patient, which greatly enhances the sensitivity of the reporting module.
For biosafety, our initial design is to prevent the leakage of the engineered bacteria by gel-embedding the engineered bacteria, but for insurance purposes, we hope to further improve safety by allowing the engineered bacteria to initiate suicide under specific conditions. We initially designed a photosensitive signaling pathway to allow the chassis cells to initiate suicide under the irradiation of blue light, which is provided by an LED in the hardware.
However, we found that this approach introduced a larger amount of genetic engineering and that actively killing the engineered bacteria with light was not as efficient as treating them directly with physical methods. So, we switched our idea and introduced a Fe3+-sensitive promoter into the toxin-antitoxin system and added Fe3+ to the gel so that the engineered bacteria leaving the gel cannot survive.
V. Hardware Design
To achieve the desired results, the hardware design focused on two main issues. The first is the choice of hydrogel material, which should be biocompatible and provide the required culture environment for C.reinhardtii; the second is how to express the feedback signal.
For the first problem, we compared various materials and chose a hydrogel material based on polyvinyl alcohol with the addition of filamentous protein and hemoglobin. This material not only ensures the normal culture of C.reinhardtii but also improves the mechanical strength of the gel due to the addition of serine protein.
For the expression of feedback signals, our initial idea was to determine the wound condition by visual observation of the color change of the dressing. Considering the needs of the elderly patient group and the fact that the wound location is mostly in the foot which is not easy to observe, we designed a wraparound brace for this purpose. Based on an everyday ankle brace, we modified it by adding flexible OLEDs to provide light for the C.reinhardtii and implanting a color recognition sensor. Since the wraparound brace provides an excellent darkroom environment, we were able to display the dressing color change on the feedback component of the brace in real time through the sensor and keep the patient informed of the wound condition through the change of light in the center of the brace and the buzzer alarm.
After solving these two key issues, we focused on the design of the dressing. We designed a three-layer structure for the dressing. The first layer is an antibacterial and waterproof PP non-woven fabric to protect the wound from external bacteria; the second layer is a hydrogel layer; and the third layer is a composite porous absorbent pad to prevent the gel liquid from spilling or embedding in the wound causing a secondary infection while protecting the skin around the wound.
Later we will focus on intelligent design and try to combine hardware and software to give real-time feedback on wound conditions to cell phones to enhance patients' experience.
There are some points in our design that have not been achieved or are temporarily difficult to achieve:
- Studies have shown that the release of too many growth factor-like substances has a cancer risk, so perhaps a negative feedback mechanism is needed to control the release of effector molecules;
- The two reporter signals are superimposed and interfere with each other, perhaps a logic gate can be designed to allow the system to generate only one reporter signal at a time.
Spreading Awareness
In order to find out how much the public knows about keywords such as diabetic foot, synthetic biology and iGEM, we designed a questionnaire, taking into account the protection of personal privacy and respect for patients, and tried to make our questionnaire gentle, valid and not offensive to anyone. We posted it on a public platform and called for people to fill it in. We were very grateful and surprised to receive 178 responses. The data from the questionnaire was tallied and we drew conclusions. These findings have helped us to design targeted Education content.
A summary of the data analysis and visualisation of the questionnaire can be found in our Education & Public Engagement section.
Conclusion &
Future Plan
We have integrated and assessed stakeholders in our integrated human practice, created a Stakeholder Map and conducted a value analysis to support the human practice. We are looking forward to connecting with more stakeholders and getting their input, and we will reinforce this in the formal project to strengthen the connection between our project and the world. At the mid-point of the project we took stock of the project and listed the experts we were looking to contact in each area and designed our interview principles, click on the attachments to view them!
Our more macro plans for the future can be viewed in our Entrepreneurship section.
REFERENCES
- [1] Fortington LV, et al. Eur J Vasc Endovasc Surg. 2013; 46(1): 124-131.
- [2] Armstrong DG, et al. J Foot Ankle Res. 2020; 13(1): 16.
- [3] Petrakis I, et al. Expert Rev Pharmacoecon Outcomes Res. 2017; 17(2): 165-180.
- [4] HSCIC. Clinical Audit and Registries Management Service. National Diabetes Foot Care Audit report 2014-2015. Report, England and Wales, March 2016.
- [5] Lim JZ, Ng NS, Thomas C. Prevention and treatment of diabetic foot ulcers. J R Soc Med. 2017 Mar;110(3):104-109.
- [6] Burgess JL, Wyant WA, Abdo Abujamra B, Kirsner RS, Jozic I. Diabetic Wound-Healing Science. Medicina (Kaunas). 2021 Oct 8;57(10):1072.
- [7] Lima AL, Illing T, Schliemann S, Elsner P. Cutaneous Manifestations of Diabetes Mellitus: A Review. Am J Clin Dermatol. 2017 Aug;18(4):541-553
- [8] Khalid M, Petroianu G, Adem A. Advanced Glycation End Products and Diabetes Mellitus: Mechanisms and Perspectives. Biomolecules. 2022;12(4):542.
- [9] Bucciarelli L.G., Wendt T., Qu W., Lu Y., Lalla E., Rong L.L., Goova M.T., Moser B., Kislinger T., Lee D.C. RAGE Blockade Stabilizes Established Atherosclerosis in Diabetic Apolipoprotein E–Null Mice. Circulation. 2002;106:2827–2835.